Depression in the workplace is more than a personal health issue – it is a significant business risk. Research suggests that untreated employee depression can cost employers around $15,000 per affected employee each year, although the true financial impact often varies by organization and is likely even higher when indirect costs are included. Those costs rarely appear on a single budget line. Instead, they accumulate through absenteeism, presenteeism, increased turnover, disability claims, reduced productivity, workplace errors, and the gradual decline of team performance. Because these losses are spread across departments and reporting systems, many organizations underestimate their impact until performance, culture, and retention begin to suffer. In this article, we’ll examine where these hidden costs come from, why untreated depression is so expensive for employers, and the evidence-based workplace strategies that help reduce both human and financial consequences.
Table of Contents
- Quick Takeaways
- The Real Math Behind the $15,000 Figure
- Where the Costs Actually Hide
- Workplace Mental Health ROI: The Business Case
- Why Most EAP Programs Fail to Move the Needle
- What Effective Employee Mental Health Training Looks Like
- Comparing Approaches to Workplace Depression Intervention
- Workplace Burnout Prevention as a Financial Strategy
- Building Mental Wealth Programs That Actually Stick
- Frequently Asked Questions
- References
Quick Takeaways
| Key Insight | Explanation |
|---|---|
| Depression costs $15,000+ per employee annually | This figure combines absenteeism, presenteeism, turnover replacement, and disability costs, most of which never appear on a mental health budget line. |
| Presenteeism outweighs absenteeism costs 3-to-1 | Employees who show up but cannot function due to depression cost organizations far more than those who take sick leave. Most organizations measure the wrong metric. |
| Untreated depression doubles turnover risk | Replacing a mid-level employee costs 50-200% of their annual salary. Depression is one of the most predictive leading indicators of voluntary resignation. |
| ROI on mental health programs averages 4:1 | According to Deloitte research, well-structured mental health interventions return $4 for every $1 invested, primarily through reduced absenteeism and improved productivity. |
| Manager behavior is the single largest risk factor | Psychosocial safety research consistently shows that how managers communicate and respond to distress determines whether depression escalates or resolves in a workplace setting. |
| EAP utilization rates average below 5% | Most organizations rely on Employee Assistance Programs that fewer than 1 in 20 employees actually use. This is not a utilization problem; it is a design problem. |
| Early intervention cuts costs by up to 40% | Organizations that train leaders to identify early signs of depression and respond appropriately reduce the average cost per case significantly compared to those who wait for formal diagnosis. |

The Real Math Behind the $15,000 Figure
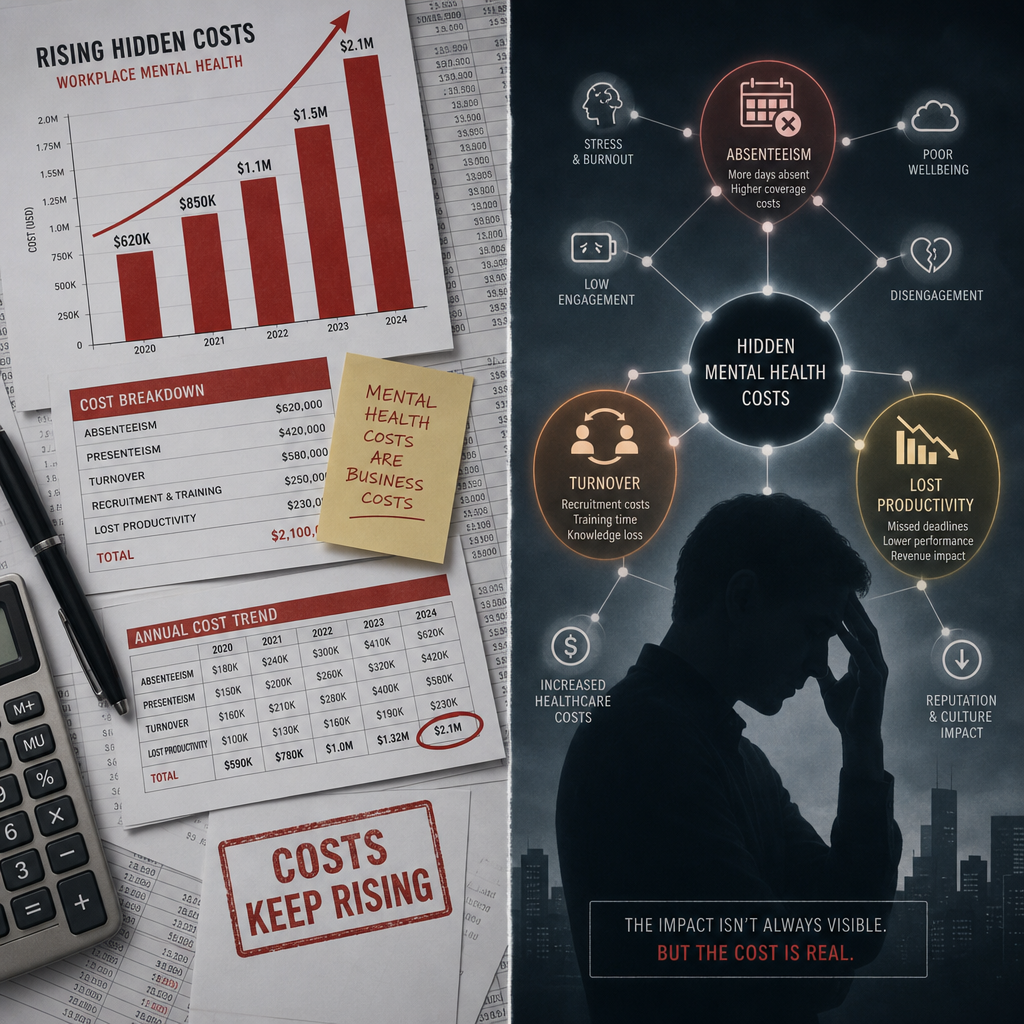
The $15,000 figure is not a dramatic exaggeration. It comes from combining multiple cost streams that organizations almost always measure in isolation. The American Institute for Stress and peer-reviewed health economics research have consistently placed the total annual cost of a single depressed employee in the range of $10,000 to $17,000 when all contributing factors are properly accounted for.
The breakdown looks approximately like this: absenteeism accounts for roughly $2,000 to $3,500 per year per affected employee. Presenteeism, which is the productivity loss from employees who are physically present but mentally impaired, adds another $5,000 to $7,000. Turnover costs, when depression is a contributing factor to resignation, add a further $4,000 to $6,000 when averaged across affected workers. Disability claims, healthcare utilization, and psychosocial injury costs make up the remainder.
The data consistently shows that organizations undercount by at least 30% because they measure absenteeism but not presenteeism, and they track turnover costs without identifying depression as a root cause.
The Presenteeism Problem That Leaders Ignore
A common mistake is focusing cost-reduction efforts entirely on sick days. Presenteeism is invisible on attendance reports, but its financial impact is three times larger. A Harvard Business Review analysis found that workers experiencing depression lose an average of 27 working days per year to reduced productivity even when they are physically present. At an average salary of $60,000 per year, that translates directly to roughly $6,200 in lost output, per person, per year.
This is the number that should be on the agenda at every executive meeting, and it almost never is.
Where the Costs Actually Hide
The cost of untreated depression at work does not arrive in a single department’s budget. It distributes itself across HR (turnover and recruitment), operations (productivity loss), finance (disability and healthcare claims), and legal (psychosocial injury claims and litigation). This distribution is precisely why it escapes scrutiny.
Recruitment and Replacement Costs
When an employee with untreated depression eventually resigns or is managed out, the replacement cost is immediate and concrete. Recruitment advertising, interviewing time, onboarding, and the productivity ramp-up period for a new hire typically cost between 50% and 200% of the departing employee’s annual salary. Organizations with poor psychosocial safety profiles see significantly higher rates of this cycle because they never address the conditions that drove the first employee out.
Disability and Workers Compensation Claims
Psychological injury claims are now among the most expensive categories in workers compensation systems across developed markets. In Australia, mental health-related workers compensation claims cost an average of $25,000 per claim, nearly three times the cost of physical injury claims, according to Safe Work Australia data. Organizations without formal psychosocial safety frameworks are statistically far more exposed to these claims.
Team Contagion Effects
Depression does not stay contained to one employee. Research published in the Journal of Applied Psychology shows that emotional exhaustion spreads through teams, a phenomenon known as emotional contagion. When one team member’s depression goes unaddressed, surrounding colleagues experience measurable declines in engagement, motivation, and performance within 60 to 90 days. The cost multiplier effect here is significant and rarely modeled by HR departments.
Pro tip: When calculating the organizational cost of untreated depression, multiply your estimated single-employee cost by 1.4 to account for team contagion effects. It is a rough but defensible adjustment that makes the business case far more compelling for executive sponsors.
Workplace Mental Health ROI: The Business Case
Workplace mental health ROI is no longer a soft argument. It is a financial calculation with empirical backing. Deloitte’s global research on mental health in the workplace found an average return of $4 for every $1 invested in mental health programs, driven primarily by reductions in absenteeism and improvements in productivity. For organizations with more than 500 employees, the dollar returns become significant enough to appear as a measurable line item in annual savings.
“The cost of not addressing mental health in the workplace is consistently higher than the cost of addressing it. Organizations that wait for a crisis to act are choosing the more expensive option.” — Deloitte Global, Mental Health and Employers Report
In practice, the organizations that generate the strongest ROI from mental health investment are not those with the most elaborate wellness programs. They are the ones that train their managers well, build psychosocial safety into team culture, and intervene early. The technology and program design matter less than the quality of implementation and the commitment from the leadership layer.
Calculating Your Organization’s Exposure
A practical starting point for any HR leader is to estimate current depression prevalence using population-level data. Approximately 1 in 5 working adults experiences a mental health condition in any given year, with depression and anxiety being the most prevalent. For an organization of 200 employees, that suggests 40 people are affected at any one time. Multiply 40 by $15,000 and the annual exposure is $600,000, before accounting for team contagion or escalating claims.
Most executive teams have never seen that number presented to them in those terms. When they do, the conversation about investment changes quickly.
Why Most EAP Programs Fail to Move the Needle
Employee Assistance Programs were designed with good intentions and have largely failed to deliver at scale. The average EAP utilization rate sits below 5%, which means that in an organization of 200 employees, fewer than 10 people are actually accessing the service at any given time. An intervention that reaches 5% of the affected population is not solving a $600,000 problem.
The reasons for low utilization are well-documented: stigma, lack of awareness, perceived confidentiality concerns, inconvenient access, and the clinical nature of most EAP services, which do not match the sub-clinical distress that characterizes early-stage workplace depression. In practice, by the time an employee calls an EAP line, the problem has already become expensive.
What EAPs Get Wrong About Timing
EAPs are reactive by design. They respond to symptoms after they have become significant enough for an employee to self-identify and self-refer. The cost of untreated depression at work is highest in the six to twelve months before an employee ever makes that call. Effective intervention needs to happen in that window, which means it needs to be delivered at the manager and team level, not through a phone line that employees associate with crisis.
Organizations that supplement EAPs with proactive manager training and psychosocial safety frameworks see utilization of all mental health supports increase, because the stigma reduces and the culture shifts toward earlier help-seeking behavior.

What Effective Employee Mental Health Training Looks Like
Employee mental health training that actually reduces the cost of untreated depression at work has three non-negotiable characteristics. First, it is psychologist-led or psychologist-designed, not outsourced to general wellness trainers. Second, it addresses managers and leaders directly, not just frontline employees. Third, it builds skills rather than raising awareness. Awareness without skills does not change behavior.
Manager Training as the Highest-Leverage Intervention
The data is unambiguous on this point. A manager’s response to early signs of employee distress is the single most predictive variable in whether depression escalates or resolves in a workplace context. Managers who receive structured training in psychological safety, early identification, and supportive conversation techniques reduce the probability of a formal mental health claim by a measurable margin.
This is not about making managers into therapists. It is about giving them a framework for recognizing change, responding without stigma, and connecting employees to appropriate support before the situation becomes a formal HR or legal matter. Programs like those offered at The Workplace Mental Health Institute structure this training specifically for the organizational and legal context that Australian and international HR leaders navigate.
Building Skills Beyond Awareness
A common mistake is treating a half-day mental health awareness session as an intervention. Awareness shifts attitudes marginally. It does not change the daily behaviors that either exacerbate or protect against workplace depression. Effective training covers specific skills: how to open a non-stigmatizing conversation, how to adjust workload and role demands for someone who is struggling, and how to document concerns in a way that is legally defensible and compassionate simultaneously.
Pro tip: When evaluating employee mental health training providers, ask for outcome data, specifically reductions in absenteeism, claims, or depression scores, from comparable organizations. Any provider who cannot produce outcome data is offering awareness, not intervention.
Comparing Approaches to Workplace Depression Intervention
Not all workplace mental health approaches carry the same cost-to-impact ratio. Understanding the differences between common approaches helps HR leaders make investment decisions that actually address the $15,000 problem rather than appearing to address it.
| Approach | Typical Cost per Employee | Evidence of Impact on Depression Costs |
|---|---|---|
| Standard EAP (reactive, self-referral model) | $100-$300 per employee per year | Low. Sub-5% utilization rates mean most affected employees are never reached. Minimal impact on presenteeism or early-stage depression. |
| Psychologist-led manager and leader training (e.g., WMHI model) | $300-$800 per manager, scalable across teams | High. Directly addresses the primary behavioral driver of workplace depression escalation. Reduces claims and turnover when implemented with fidelity. |
| Generic wellness app or digital platform | $50-$150 per employee per year | Minimal for depression specifically. Useful for general wellbeing and resilience but lacks the clinical rigor and manager-level intervention needed to reduce serious depression costs. |
The table above reflects a consistent pattern: the interventions with the strongest evidence base are those that operate at the manager and organizational culture level, not those delivered as individual tools to employees who are already struggling in silence.
Workplace Burnout Prevention as a Financial Strategy
Workplace burnout prevention and depression prevention are not identical, but they share enough causal pathways that investment in one protects against both. Burnout, characterized by exhaustion, cynicism, and reduced professional efficacy, is a direct precursor to clinical depression in a significant proportion of cases. The World Health Organization formally classified burnout as an occupational phenomenon in 2019, and the financial consequences have been quantified repeatedly since.
Organizations that implement structured burnout prevention, including workload audits, role clarity initiatives, and psychosocial hazard assessments, report measurable reductions in both depression-related absenteeism and psychological injury claims within 12 to 18 months of implementation. The investment required to conduct a proper psychosocial safety assessment and act on its findings is typically recovered within the first year through avoided claims alone.
Psychosocial Hazard Identification
Most organizations have robust processes for identifying physical hazards in the workplace and almost no equivalent process for psychosocial hazards. Psychosocial hazards include excessive workload, low role clarity, poor leadership behavior, lack of autonomy, and organizational injustice. These are the conditions that breed both burnout and depression, and they are measurable, manageable, and legally relevant in an increasing number of jurisdictions.
In Australia, the model Work Health and Safety laws were updated to explicitly include psychosocial hazards as employer responsibilities. Organizations that have not conducted a formal psychosocial risk assessment are not just leaving money on the table; they are carrying legal exposure they may not have quantified.
Building Mental Wealth Programs That Actually Stick
Mental wealth programs are a framing shift that matters. The term “mental health” carries clinical connotations that can trigger stigma and create a barrier to engagement, particularly among high-performing employees who resist identifying as struggling. Mental wealth reframes the conversation around building psychological resources, resilience, and organizational capability rather than fixing deficits.
In practice, mental wealth programs that achieve sustained adoption share several structural features. They are embedded in regular organizational rhythms rather than delivered as isolated events. They create visible leadership commitment at the executive level. They include measurement and reporting so that outcomes are tracked and improvements are recognized. And they build internal capability so that the organization is not permanently dependent on external providers for maintenance.
Resilience Building as a Measurable Organizational Asset
Resilience is not a personality trait that some employees have and others do not. It is a set of cognitive and behavioral skills that can be taught, practiced, and embedded in team culture. Organizations that treat resilience building as a competency development initiative, with the same rigor applied to technical skills training, consistently outperform those that treat it as a motivational exercise.
The measurable outcomes of properly designed resilience programs include reductions in sick day frequency, improvements in team cohesion scores, reductions in voluntary turnover, and in longitudinal studies, measurable reductions in self-reported depression symptoms. These are outcomes that HR leaders can report to executive teams with confidence.
The organizations that fail with resilience programs are almost always those that deliver a single workshop and measure nothing afterward. The organizations that succeed treat resilience as an ongoing organizational competency, reviewed quarterly and reinforced through manager behavior and team practices.
Frequently Asked Questions
How is the $15,000 cost per depressed employee calculated?
The figure combines four cost streams: absenteeism (lost days due to depression-related sick leave), presenteeism (productivity loss while present but impaired), turnover costs (when depression contributes to resignation or termination), and disability or psychological injury claims. Most organizations only measure absenteeism, which means their true cost per affected employee is substantially higher than they realize. The $15,000 estimate is conservative for mid-to-senior roles where salary levels are higher.
What is the difference between burnout and depression in a workplace context?
Burnout is classified as an occupational phenomenon driven by chronic unmanaged workplace stress. Clinical depression is a medical condition with broader causes and symptoms. In the workplace, they overlap significantly. Burnout that goes unaddressed commonly progresses into clinical depression. From a cost perspective, both produce the same financial outcomes: absenteeism, presenteeism, turnover, and claims. Workplace intervention strategies that address psychosocial hazards, which drive burnout, also serve as protective factors against depression.
What should HR leaders look for when choosing an employee mental health training provider?
Three things matter most. First, the program must be psychologist-designed or psychologist-led, not delivered by general wellness coaches without clinical training. Second, the provider must be able to demonstrate outcome data from comparable organizations, including reductions in absenteeism, claims, or validated psychological distress scores. Third, the program must include manager and leader training as a core component, not an optional add-on. Awareness programs without behavioral skill components do not produce measurable cost reductions.
Can small and mid-sized organizations afford mental health training programs?
The more relevant question is whether they can afford not to. For a 100-person organization with a conservative estimate of 15% depression prevalence, the annual cost of untreated depression exceeds $225,000. A structured manager training program and psychosocial safety assessment typically costs a fraction of that figure and produces measurable returns within the first financial year. Organizations that frame mental health training as a cost rather than an investment have not done the full cost-benefit calculation.
How long does it take to see ROI from workplace mental health programs?
Well-designed programs typically produce measurable outcomes within 6 to 12 months of implementation. The fastest returns come from reductions in absenteeism, which are trackable on existing HR data systems. Reductions in turnover and disability claims typically take 12 to 18 months to appear in the data. Improvements in productivity and engagement, which represent the largest component of the financial case, are measurable through existing performance and engagement survey data when baseline measurements are established before the program begins.
Is psychosocial safety legally required in Australia?
Yes, and the regulatory environment is tightening. Following model Work Health and Safety law amendments, Australian employers have explicit duties to identify and manage psychosocial hazards in the same way they manage physical safety risks. Failure to do so creates legal exposure to psychological injury claims and regulatory action. This is not a future consideration; it is a current compliance requirement that many organizations are only partially meeting.
Have you calculated what untreated depression is actually costing your organization, and what surprised you most when you looked at the full picture?
References
- McKinsey Global Institute research on workplace mental health costs and productivity impacts
- World Health Organization data on depression as a leading cause of workplace disability globally
- Forbes reporting on the financial ROI of corporate mental health investment programs
- Statista statistics on employee mental health, absenteeism, and workplace wellbeing trends
- Centers for Disease Control and Prevention data on depression costs to employers and the U.S. workforce

